July 27th – 28th 2023 saw the PNG Society for Rural and Remote Health executives convene for a strategic planning meeting. As this executive’s term comes to an end this September, they had identified the need for a distinct vision and clear road map to guide future executives to achieve that vision.
L-R: Dr Imelda Assaigo (Society Officer), Dr David Mills (Founder), Dr Spencer Kimsen (Secretary), Dr Varghese Philip (Facilitator), Dr Camy Thomas (Treasurer), Dr Hogande Kiafuli (President)
The Society was created in 2009 and for the next 10 years the same president, founder Dr David Mills, was re-elected every 2 years. This provided for continuity, stability, and growth. However, since 2019 the executive leadership has changed twice.
The Society has also grown greater than an annual continuing medical education conference for its members, the need for this road map became inherently obvious. Each executive term is only 2 years which created hurdles in starting a project and not necessarily see its completion.
The PNG Society for Rural and Remote Health has over the past 14 years established itself as a professional society and has seen the need to expand our work more dynamically in other areas as mandated through our constitution.
Looking towards the future we hope to further develop our advocacy and awareness arms to boldly drive for quality health service in rural areas and spotlight rural health issues at local and national levels, to the public and the government. We want to continue to nurture our members through providing continuing learning and improvement conferences or platforms, and creating arenas of community, encouragement, and support.
To achieve all this a plan was needed and is now here!
July 11th this year the Rural School branch of the School of Medicine and Health Science (UPNG) was officially launched. The Rural School is incorporated as part of the Kompiam District Hospital in Enga. Sitting down with Dr David Mills later that month he shared how this dream of a medical school based at a rural health facility began 6 or 7 years ago. He had set aside some land and proposed the project to the dean of the School of Medicine and Health Science, UPNG. However, it took some time and after about 4 years of planning then 2 years of construction the rural school was formally opened.
Official Opening Ceremony
The first group of 8 students arrived in June to complete the remaining components of their final year of medical school. These last two components of their training consist of Maternal and Child Health as well as Rural Health. Their colleagues remain in Port Moresby at the Medical Faculty, Taurama Campus. For these 7 students being situated at Kompiam already fulfils the ‘rural health’ component and the maternal plus child health module will be completed through rural patrols to neighbouring health centres as well as participating in the well-baby and maternal health static clinic at the Kompiam Hospital.
MBBS 5 UPNG Students
The students were not chosen at random, but each requested to go and were selected from the multiple essay applications. 2024 will see the first group of 5th year medical students who will complete the entirety of their final year of medical training at the rural school. Much like the traditional schooling format the students have access to didactic teaching as well as the classroom experience however this will now be provided via Wi-Fi from the Medical Faculty. They will have the same classes and teaching as their colleagues but instead of urban clinics and PMGH based medicine these students will experience and contribute to the health and wellbeing of the rural population of Kompiam district. They will learn what rural health in Papua New Guinea actually comprises of, and see the strength of will and resourcefulness that is required to provide quality health care to all our people of Papua New Guinea.
Study station for StudentsWi-fi classroom – set up for lecturesConference facility
Dr Hogande Kiafuli presenting the Recommendations of Rural Hospital Design to Deputy Secretary Dr Lenturut
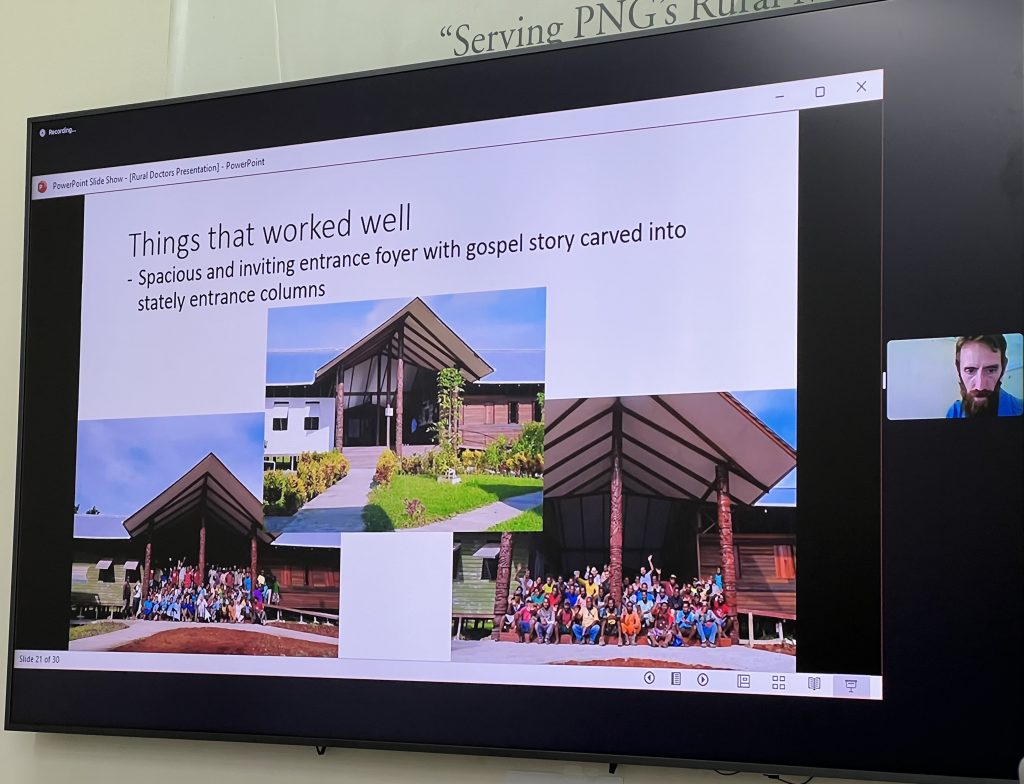
In 2022 PNG Rural and Remote Health Society annual symposium theme was Rural Hospital Design – Should There Be A Minimum Standard?
The symposium which took place in September last year had speakers from various rural hospitals throughout the country share their experience of their individual hospital design successes, flaws and lessons learnt. The islands perspective was shared by Dr Siaol Panta based on Misima Island, the highlands view from Dr David Mills of Kompiam and the coastal insight from Dr Valerie Archer based at Kapuna. Dr Ambrose Kwaramb, the Manager for Building and Facility Standards of the National Department of Health opened the meeting giving the national position in terms of healthcare facilities infrastructure standard, planning, design, delivery and sustainability. We gleaned an international viewpoint from guest speaker Dr John Oomen, the medical superintendent of Christian Hospital Bissamcuttack and his 30yrs experience working in the rural and remote communities in India.
Dr Ambrose Kwaramb, Manager for Building and Facility Standards, National Department of HealthDr Sialo Panta, MMed Rural Medicine Registrar, based at Misima IslandDr Valerie Archer, Medical Director, Kapuna District Hospital, Kapuna, Gulf ProvinceMr Marshall McKean, Project Manager of Kapuna Hospital Rebuild. Presenting via Zoom.
These talks set the stage for the interactive discussion between the society members as well as the non-members who were themselves past or current practitioners in rural hospitals; as to what is and how should a rural hospital in Papua New Guinea be designed. These thoughts were complied into – Principles of Rural Hospital Design, Recommendations on NHS Design Standards, and presented to Dr Lenturut of the National Department of Health on 2nd June during the National Health Service Standards conference in Mt Hagen.
When Dr Kiafuli, president of the PNG Society for Rural and Remote Health, was invited to speak at the Christian Health Services Annual General Assembly on 27th April 2023 he used the opportunity to introduce initiatives to engage and retain doctors to the rural and district hospitals. Many of the health facilities operated by the Christian Health Services member organisations are in rural and remote areas of Papua New Guinea. They all know the struggle it is to recruit let alone keep a doctor in their health facilities.
With the CHS recently being incorporated into the government Alesco payroll system Dr Kiafuli stressed that key factors for doctors serving in rural facilities was more than money. Although a salary and benefits package offered to be on par with their public sector colleagues was helpful to retain the doctor for the long term factors such as:
professional development
financial incentive
job satisfaction
social amenities
In Dr Kiafuli’s own words he summarised it thus:
“In a scoping review of various qualitative studies conducted all around the world, four themes are identified as primary factors that promote recruitment and retention of doctors in the rural areas.
Professional Development This factor tops the list of factors motivating doctors to remain and serve in the rural areas of their respective countries.
Post-Graduate development Most doctors have a drive to acquire further qualifications after their basic graduate degree (MBBS). The employer must be able to nurture that drive so they will have a higher chance of retaining the doctor.
The PNG Society for Rural & Remote Health is a strong advocator of the Master in Medicine (Rural Health) post-graduate course offered at UPNG. This course gives a strategic advantage to PNG employers to recruit and retain doctor in the rural areas. It is designed in PNG, and for PNG and has few notable advantages:
It provides a curriculum drive to retain a medical doctor in the rural hospital for at least six years.
It provides a curriculum structure that trains the type of rural generalist well suited to PNG setting, who could take on a wide variety clinical cases, contribute to leadership and management and advise on quality improvement and infrastructure developments.
It provides a curriculum content that elevates the candidate to the master-level comparable to other master of medicine training. It gives no room for any well-informed person to accuse Rural Medicine as low-quality or boring speciality.
Some doctors may serve in rural hospitals but will choose against take the Rural Medicine course offered in UPNG. It is entirely up to them, and the respective employer can formally agree to sponsor for other course per individual doctors’ preference. Sponsoring doctors for in-person courses offered internationally carries the disadvantage of the doctor being absent from the hospital for 1 – 2 years.
Continuing medical education (CME) Apart from post-graduate qualifications, good and consistent continuing medical education support does score points in favour of retaining medical doctors in the rural areas. Each employer and their respective medical officers can communicate regarding options for that but common CME avenues to consider include:
Annual Medical Symposium organized by the Medical Society of PNG
Specific and relevant medical conferences organized anywhere in the world.
Short courses/trainings organized by PHAs or professional Societies, including PNG SRRH
Subscription fees to receive access to articles in renown medical journals.
Financial Incentives Providing good financial incentives for doctors who work in the rural areas is, in all countries, a paramount force of retention of doctors in rural hospitals. Employers will need to be smart and creative about how to go about addressing this. Financial Incentives may take different forms:
Higher salary grade. For rural hospitals in PNG, we recommend that salary grade 14 should be the minimum for doctors living and working in the rural hospitals. This is particularly important when the doctor is also taking the rural medicine training at UPNG.
Higher duty allowances can be given to doctors taking up leadership roles in the rural hospitals but this will largely depend on the positions to which they are contracted for, and whether provision was made for higher duties in the contract.
Cash incentives have been made possible by partnership with DDAs and provincial governments, but may not be possible in all setting.
Job Satisfaction A doctor who is not satisfied in the everyday performance of duty may be difficult to retain. Factors promoting satisfaction in the workplace include a supporting clinical and administrative team. A particularly bottle-necked management will greatly injure work satisfaction of the doctor. Facilities poorly resourced will also reduce work satisfaction. On the other hand, a very supportive agency or political management can often encourage a doctor to improve resources, which will increase satisfaction for the efforts input. It is vital for agency managers to embrace effective communication and teamwork with their medical workforce. Unity and teamwork are a strength to be nurtured.
Personal Satisfaction. Although not uniformly reported as a motivating factor, observations have been made that doctors that feels respected and appreciated by the community, hospital team and the respective management, will be satisfied with the social environment of the workplace.
Social Amenities Providing good housing with reliable water and power is also a vital force for retention of doctors in the rural hospitals. Ease of access to banking services, and availability of quality school for their children are amenities that promote retention (their absence reduces the chances of retaining a doctor in the rural hospital). The provision of these amenities will need good partnership with relevant stakeholders. In particular, the political leadership of the respective districts are major players to assist with provision of these amenities. “
Dr Kiafuli then identified ways in which these recruitment and retention factors could be implemented right now in Papua New Guinea today, titled Way Forward
WayForward
Policy for Retention The Master of Medicine (Rural Health) training is able to attract and retain doctors in the rural areas through a curriculum drive. There is a potential for a equally stronger drive from policy specifically on the recruitment and retention of doctors in rural areas.
Flexible Positions The medical officer positions from CHS agencies absorbed into Alesco payroll need to be flexible enough to recruit Rural Medicine trainees in the respective rural hospitals. This is particularly true for the SMO positions – they need to be flexible enough to employ trainee registrars against that position. The CHS Secretariat has assured that because the positions are ‘living’, and can be reviewed every two years, this will not be a significant problem.
PHA Support While some rural hospitals are being well supported by their PHAs, some have received little or no support at all. It is disheartening to see different support level given to respective rural hospitals and their medical officers. The Society calls for an evaluation of each PHA by the National Health Department, to set a guideline (or even a policy) for each PHA in how they can support their district hospitals.
Current President of PNG Society for Rural and Remote Health, Dr Hogande Kiafuli, presents Dr David Mills with a bamboo burnt art piece in thanks for all he has done for medicine, in particular rural medicine, in Papua New Guinea
Recognising the immense contribution of Dr David Mills, the founder of the PNG Society for Rural and Remote Health as well the instigator plus engineer of the Masters in Rural Medicine (UPNG) program.
As many gathered to farewell the Mills family at Kompiam on Saturday 26th November our present president reflects the following:
Jimi district in Jiwaka province is one of the most remote in Papua New Guinea. I travelled to Middle and Upper Jimi on my way to Kompiam this weekend and experienced firsthand the struggles of accessibility that the people of Jimi have when it comes to accessing primary medical services.
Jimi district represents the many rural and remote (and some isolated) places in Papua New Guinea where accessing primary medical care is limited by poor road access; where winding and narrow is the path to accessing a doctor; where pastures of medical care is brown. The government of Papua New Guinea has tried various approaches to solving this issue but all seemed to be superficial, symptomatic and reactive solutions.
There needed to be a change of approach – a paradigm shift. A systemic approach that foster unity of influence; a systematic approach that ensure uniformity amongst diversity; a synergistic approach that bonds vital parts for a better whole. A shift from reactive to proactive. If the people are unable to access a doctor, then let us enable the doctor to access the people.
God’s will to improve rural medical health in Papua New Guinea was instilled as a vision in David Mills and his family. With grits, guts and grind, but most importantly God, the family relocated from Australia, the land down under, to Kompiam District in Enga Province, a land out further. They came as missionaries, and visionaries, carrying seeds of change from God that will transform rural medical service in Papua New Guinea.
One seed was planted in the fertile soils of Kompiam Health Center. Out sprouted the now blossoming tree of Kompiam District Hospital, which is one of the best rural hospitals in Papua New Guinea. A second seed was planted still at Kompiam, where it now is blooming as Kompiam International School, providing quality education in a rural district.
The next seed was planted at the University of Papua New Guinea (UPNG). This was a very special seed – unique in the world and found only in Papua New Guinea. It germinated with struggle but was nurtured passionately till it bloomed into a specialist training program, which has yielded seven master of medicine specialists, specialising in rural health. As it branched further, the Department of Rural & General Medicine took emerged and is now an important department in the UPNG School of Medicine.
Another seed was planted in Papua New Guinea as the PNG Society for Rural and Remote Health. It too struggled to grow but did so eventually and is now a place for rural doctors to ‘feel at home’.
These seeds are actually smart strategies to obtain, maintain and retain doctors in the rural areas. Sure enough, we have a Department that attracts medical students into rural medicine; a graduate level Curriculum that keeps rural registrars in rural hospitals; and a professional Society that keeps the rural doctors connected.
If we are a Society of painters, we would paint a thousand pictures to speak ten thousand words of gratitude to the Mills for their passion, dedication and perseverance in improving rural medical services. They heeded to the call of God and allowed the Holy Spirit to use them to initiate, influence and impact a paradigm shift. Rural medical services is a better version now!
Prosperity is when your life becomes a blessing and healing to others. The Mills have lived a life of prosperity and we wish them more prosperous times ahead and abroad.
On behalf of a grateful Society, and a grateful nation.
Dr. Hogande Kiafuli President – PNG Society for Rural and Remote Health.
Dr Kiafuli visiting Wara Mantz CHP facility under the EBC Church in the Middle Jimi area of the Jimi District in Jiwaka. En route to Kompiam to farewell Dr Mills.